In the last year, I have delivered three presentations on culture, race and health inequalities to physiotherapists and AHPs. In my talk I describe how early on in my career, I assimilated into the culture of the Physiotherapy profession and department I worked at the expense of my ethnic minority identity. I was less confident as a an individual and professional, desperate for acceptance in the team. I had a lightbulb moment a few years later and started to see what was problematic in our profession.
Let’s rewind and explore definitions:
Culture is… a set of guidelines… which an individual inherits as a member of a particular society and which tells him [sic] how to view the world and learn how to behave in relation to other people (Helman, 1994)
Culture in its broadest sense is cultivated behaviour; that is the totality of a person’s learned, cultivated experience which is socially transmitted, or more briefly, behaviour through social learning.
I realised early on in my career how physiotherapists were meant to behave: efficient, outspoken, tough and resilient, physically robust, social. Even as a student I quickly caught on that socialising within teams centred around sharing food and going to the pub. Not an immediate problem for me as my cultural upbringing does not exclude drinking alcohol but reflecting back I can start to see where those exclusions start to bite for people not from the dominant culture.
Health institutions have a particular culture. The fast pace of an acute hospital, a community team: there will be expectations of the behaviour of people working within them. The expectation of the workforce is one thing, but what about if there are expectations of the people accessing those services? Of how they should behave? Or even how they should look? When all of our anatomy books, physiotherapy texts, even exercise prescription tools show white bodies. European expectations underpin our learning and our skills development.
There are things that have been normalised in the Physiotherapy professional culture. Here are two examples: undressing for practical learning and using touch in our therapeutic interactions. On the surface nothing may spring to mind that is problematic about either of those things. “We’re physios. It’s how we were taught! It’s what we do!” I’ll delve deeper with a couple of stories:
• Undressing to shorts and vest for practical sessions:
I was a lecturer for 11 years in an inner-city university in a diverse area. Colleagues were getting ready for practical sessions for the first years when they reported back in a staff meeting that there was a problem. A handful of students were Muslim and did not want to undress in front of peers in mixed classes. Colleagues thought this was detrimental to the learning of the whole group and were astonished that they did not realised this was what physiotherapists did prior to applying. Where did that assumption come from? Why is there that expectation? Where is it written down? Is it really so vital to learning in that format? It was a very difficult, heated meeting and the upshot was, it was left to me and another BAME member of staff to come up with a solution. What does that tell you?
• Using touch in our therapeutic interactions
I recall a time when I was a young neuro-physiotherapist, fresh from my three-week Bobath course, armed with some new handling techniques to try out on my stroke patients. One technique taught by the tutors to facilitate hip extensor activation was sitting in front of the patient on a stool, helping the person up into standing, placing an arm through their legs so the therapist’s hand could be placed on the posterior part of the pelvis on the weak side (the buttock) to help facilitate posterior pelvic tilt and activate the gluteus maximus. It worked really well in the practical session, but when I was sat in front of a patient a few days later, I realised the inappropriateness of this technique in the context I found myself. It can be argued that such a technique is invasive for anyone, but this is what we were taught.
The older Asian gentleman in front of me on the plinth made me stop in my tracks. In Asian culture, older Asian men will treat you as one their own, often calling you “betee” (daughter) even beyond extended family. Modesty and dignity are also paramount. I was suddenly very aware that if I handled him in the way I was taught, it would be particularly shocking and humiliating for him to be touched in that way by a younger woman. I was able to work with him to achieve good results in a different way that did not involve crossing those boundaries of dignity. My cultural sensitivity in that situation was because of my upbringing. I was the only BAME member of the team so others may not have had cultural competence to come to the same realisation.
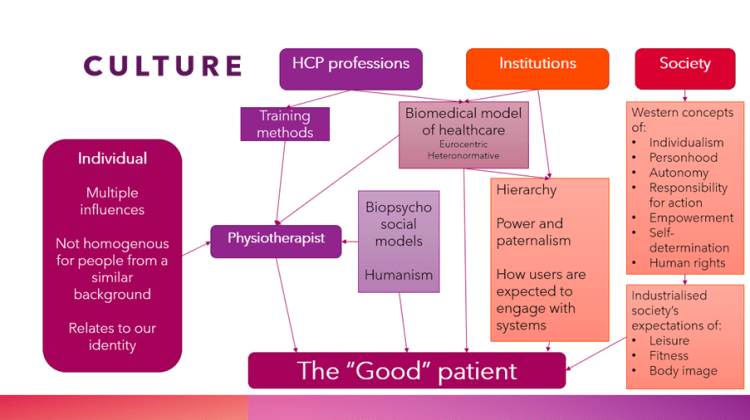
I and others have witnessed and explored a culture clash between physiotherapeutic treatment approaches, acceptable within the culture of the profession, and the culture of the people we are serving. This is because the profession lacks cultural literacy due to the Eurocentric frameworks we are educated in, and there is also limited understanding beyond heteronormativity.
My musings are not new and culture in our profession was explored in the late 2000s through a handful if papers on the topic (Norris and Allotey, 2008; Hunt M, 2009; Remedios et al. 2009). I would like to think we have learned from these papers, but unfortunately, I still witness health inequalities where a clash of professional and individual culture could be a factor. We can be quick to label a patient as non-compliant, not engaging, and lacking rehabilitation potential because they do not fit neatly into our expectations of “the good patient”. When there isn’t a neat intersect between the culture of the physiotherapist, culture of the institution they work in and the culture of the patient, the patient is the one who risks exclusion. Did we take the extra effort to listen to their concerns, and understand where there may have been anxiety about what we are proposing? Have we lost the trust of a proportion of our patients?

I have recently highlighted on social media situations where the culture within departments can also be affecting the experience of BAME colleagues. I am hearing multiple stories of colleagues being leapfrogged for promotions and denied training opportunities. Comments made about accents, certain black hairstyles being unprofessional, colleagues working at a far lower level than they did in their home country. I have seen those cliques in departments in my 26 years as a physiotherapist. I have heard the resounding silence when inappropriate comments have been made by senior, charismatic leaders. This is now. The profession needs shaking up and colleagues need to see, to hear that it is not welcoming to all and can exclude a proportion of the people we serve.
I am ducking at the expected backlash as I write this, but we should all be working to change the physiotherapy culture to one where diversity does not cause controversy, inclusion is automatic, and equity of opportunity is there for everyone.
Further reading:
Hunt M. Taking culture seriously: considerations for physiotherapists. Physiotherapy 2009; 93: 229-232
Jaggi A and Bithell C. Reltionaships between physiotherapists’ level of contact, cultural awareness and communication with Bangladeshi patients in two health authorities. Physiotherapy; 81:330-7
Norris M, Allotey P. Culture and Physiotherapy. Diversity in Health and Social Care 2008; 5:151-9
Remedios L, Dawson H, Edwards I. Ch. 10: Culture and Physiotherapy Practice in Contexts of Physiotherapy Practice, Eds Higgs J et al. 2009, Churchill Livingston, NSW, Australia
